FILE - In this 1950's photo made available by the National Archives, a man included in a syphilis study has blood drawn by a doctor in Alabama. For 40 years starting in 1932, medical workers in the segregated South withheld treatment for Black men who were unaware they had syphilis, so doctors could track the ravages of the illness and dissect their bodies afterward. (National Archives via AP)
In 2018, an African American woman was in the hospital as she was about to give birth to her first baby. She was in near perfect physical condition, and her medical complications were treatable if addressed early and efficiently.
When she talked to the nurse about the pain she was experiencing, the nurse commented that it was probably the medications making her confused and she ought to go back to bed. Eventually, the doctor came into the room and addressed the issues. The baby was born healthy, but the patient suffered short-term consequences, all as a result of the nurse failing to believe the patient.
The patient in the story is Serena Williams, the famed and dominant tennis superstar who gave birth to her child nearly five years ago.
This story is not unique to medicine, as there is a researched and proven history of the frequent disbelief of the reported pain of African American patients when speaking with white physicians.
Such brings us to our topic of consideration for today: inequalities in healthcare.
The role of ethnicity in health inequality
As I noted in “What does it truly mean to be pro-life today?,” being pro-life is more than opposing abortion; it ultimately revolves around cultivating a culture of flourishing life.
The American population’s health is not monolithic. The level of education, income level, and even zip code dictate the different healthcare standards and outcomes a person experiences.
While each category deserves its own attention as to reasons why and what responsibility Christians owe to alleviating those disparities, there is one category I wish to focus on today: ethnicity.
The concern about the role of ethnicity within the American healthcare system is twofold.
A tragic example of health inequality in the US: The Tuskegee experiment
First, for a majority of its history the American system of medical research has relied on the coerced bodies of enslaved persons and African Americans in the hopes of discovering a cure or developing a beneficial procedure.
There are books to be written about the history of abuse in medical research. (In fact, there have been, such as Medical Apartheid, a helpful resource and starting point.) But for purposes of conciseness, we will limit the conversation concerning one horrific example.
In 1932 in Macon, Alabama, the Tuskegee Institute—a teaching institution started in the late 1800s with Booker T. Washington as its first teacher and later became Tuskegee University—began tracking syphilis among the African American male population. There were more than 600 men involved in the study: 399 had the disease while 201 were kept as a control group.
The men were lured into the study with the promise of free transportation, meals on study days, and free medical treatment for minor medical issues. Among a majority sharecropping population, this offer was nearly irresistible. The conditions presented made it almost impossible for the research participants to offer their consent due to the researchers’ extortionate offer.
The study commenced and continued for more than ten years, largely unfettered. In 1943, penicillin was made widely available, a cheap and effective cure for syphilis. However, the men afflicted with the disease were not offered treatment. In fact, the researchers continued with their research as planned, allowing these men to die of a curable disease.
The study persisted until 1972—yes, 1972—until the Associated Press broke a story about the study and their prolific abuse of African American men. The study quickly ended, and in 1973 a class-action lawsuit was filed on behalf of the men.
The repercussions of this study, in concordance with numerous other studies of abuse (profiled in groundbreaking articles such as this), have caused a significant amount of cultural mistrust among African American populations toward the medical profession. The results of this distrust are calamitous.
One consequence of such distrust is that when medical attention is needed, the likelihood that treatment is sought out is greatly diminished. In short, the effect is that a whole population group is afflicted and struggles with illnesses and diseases that are manageable, controllable, and treatable. The solution to this quandary is not to simply get African Americans to the doctor more often but to address the historical malpractice of medicine where the solution benefits generations of persons to come.
The disproportionate effect of medical inequality on people of color
The second issue of the role of ethnicity across the healthcare landscape is the disparate outcomes noticed today.
While each of these differences has a historical, social, and structural explanation, I will simply highlight some of the alarming numbers research produces:
- African Americans are “30 percent more likely to die from heart disease than non-Hispanic whites.”
- “African American women are nearly 50 percent more likely to have high blood pressure, as compared to non-Hispanic white women.”
- “Pregnancy-related mortality rates among Black and American Indian and Alaskan Native women are over three and two times higher, respectively, compared to the rate for White women.”
- “Eighty percent of African American women are overweight or obese compared to 64.8 percent of non-Hispanic white women.”
- “Approximately 25 percent of Hispanics have high blood pressure.”
- “In 2017, the number of suicide attempts by adolescent Hispanic females was 40 percent higher than that of adolescent non-Hispanic white females.”
- “In 2017, 7.3 percent of Asian Americans were uninsured compared with 5.9 percent of non-Hispanic whites.”
- “6 percent of Asian American adults received prescription medications for mental health services compared with 15.4 percent of non-Hispanic white adults.”
- “In 2016, Native Hawaiians and Pacific Islanders were 80 percent more likely to be obese compared with non-Hispanic whites.”
What contributes to the disparity?
6 causes for health disparities in the US
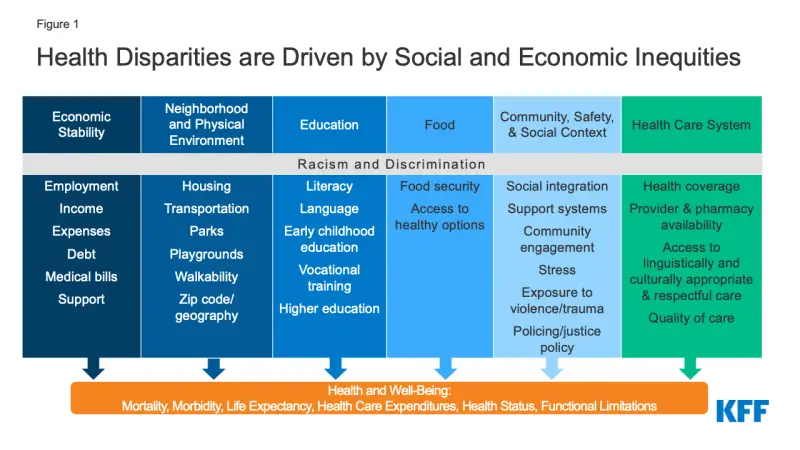
Figure 1: Health Disparities are Driven by Social and Economic Inequities | KFF
The answer is complex and multifaceted. By reading through the graph provided by the Kaiser Family Foundation, there are six distinct causes of such disparities.
Each cause is unique, but they work together to create a robust web, compounding into a problem to be solved with attention to its multifaceted influence of factors.
What should a Christian’s response to these maladies be?
How should Christians seek health equality?
As I am writing this, I am sitting at a conference on the role of religion in medicine, having just listened to my friend present about virtue ethics. Given the topic is top of my mind, what Aristotle says about the virtue of justice is a helpful beginning place.
For nearly every virtue Aristotle names—courage, friendliness, modesty, etc.—there is both an excess and a deficiency to each. However, when Aristotle speaks about virtue, he says that the virtue of justice can never be in excess; in essence, each person ought to strive to be more just every day, in every action.
To address health disparities in our communities, the work requires cooperation, persistence, and a commitment to endurance. The issues cannot be solved overnight; they are issues for a lifetime.
Further, some of the issues that affect populations mentioned above require complex, intricate solutions that can only be developed and implemented by highly trained medical and policy professionals.
Recognizing this, I propose three helpful steps that each Christian can follow to begin the work of promoting justice within each of our communities.
1. Education
Education about prevailing issues is important. This step is admittedly the easiest and can occur at your own pace and on your own time. Education happens by reading articles like these and books like the one linked above and other sources (a comprehensive list can be found here).
2. Personal engagement
Regardless of where each person lives, most likely there is a Christian nonprofit or church already working to address a specific health issue in your town. Rather than starting a new organization with its own mission (though sometimes needed), most of the time it is more helpful to the struggling populations to join an already existing support network.
Practically, crisis pregnancy centers, street medicine clinics, or something as simple as a community garden in a food desert offer significant opportunities to close health disparity gaps.
3. Church action
In the ’90s, Pastor Kyle Childress—pastor at Austin Heights Baptist Church, at the time a Southern Baptist Church—began a ministry within their church to assist the large HIV/AIDS populations that were underserved in their community. They did not offer medicine, but their action still addressed health disparities. Instead of medicine, they offered food, blankets, and hospitality to a population facing prolific discrimination.
The story of Austin Heights can be the story of churches across the country. All it requires is an awareness of a prevailing issue and a few church congregants willing to address the issues they see.
A concise biblical argument for health equality
To believe that the sum of closing health gaps is prescribing medicine is erroneous. Rather, providing material goods to promote flourishing and to alleviate the suffering of persons in our communities is a wonderful place to begin.
Further, you might have noticed, there is a lack of biblical evidence throughout this article. Such is the case for one reason.
In Matthew 25, Jesus is speaking to a small crowd and offers clear, literal teaching on the shape of a life following Christ. In verse 26, Jesus says, “I was sick and you looked after me.”
In this simple clause—it is merely listed within a sentence of other commands—we find a Christian ethic for medicine. At its root, the Christian is to care for those who are ill, suffering, and sick.
Given the realities we address each day, there needs no more explanation than the eight words Christ offered for the Christian to become involved.
Our world is suffering, and we can and must assist.
Let us act in obedience and follow in the way of Christ.
This article is part five a six-part series on “6 topics in biomedical ethics every Christian should be concerned about.”